
Central Basildon PCN in Essex is one of the 10 networks shortlisted for PCN of the year. By treating clinical and non-clinical challenges together, the PCN has reduced demand on GPs while improving outcomes for patients. PCN clinical director Dr Subrata Basu, PCN manager Carol Teatino and PCN digital lead Thanuya Mampilly explain more.
With a patient population of over 50,000 across nine practices, Central Basildon PCN was grappling with rising demand amidst dwindling GP numbers and increasing A&E attendances.
The problem was a patient population that faced significant health inequalities. Across the PCN, many patients from the BAME community live in some of the most socioeconomically deprived areas of Essex.
To better understand what was going on, we conducted a data deep-dive of three practices – accounting for one fifth of the PCN population - in September 2022.
It revealed that a significant proportion of frequent users of both GP and emergency services were the same individuals. They were predominantly aged 15–45 and experiencing anxiety and depression due to complex social stressors. More than 80% were already prescribed mental health medication.
It was clear that a more integrated, community-focused approach was needed - one built on trusted relationships across general practice and social care, community and voluntary services.
What we did
We wanted to provide equitable care that met the complex and evolving needs of our diverse population. So, when we established an Integrated Neighbourhood Team (INT) in February 2023, we adopted a culturally sensitive model of care with a particular focus on highly deprived areas.
Recognising the importance of cultural and religious context, we engaged with community leaders and faith groups to build trust, improve access and tailor support to the needs of patients, especially young adults with mental health needs.
We hoped that a multidisciplinary framework would break down traditional silos, and we leveraged existing roles - ARRS-funded care coordinators – to act as a bridge between primary care and voluntary sector services.
Our INT brought together GPs, mental health practitioners, care coordinators, social prescribers, and representatives from social care and housing. Weekly multidisciplinary team (MDT) meetings enabled joint discussion of complex patients, coordinated care planning, and ensured no one slipped through the gaps.
Mapping services
The INT team has worked cohesively to deliver proactive, personalised care that reduces dependency on primary care and emergency departments.
A key innovation has been our dedicated care coordinators who act as the central link between patients and services. We started with one care coordinator and later increased to two.
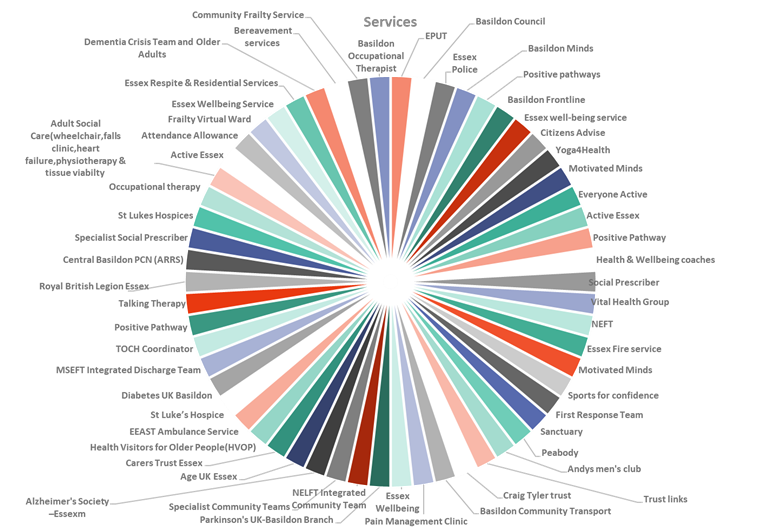
At the outset, we mapped local services, many of them previously unknown to us. Care coordinators liaised directly with over 60 providers, such as mental health organisations, safeguarding teams, housing and benefits advisors, and youth engagement services.
By creating a network, we ensured patients could access personalised support. Instead of being passed between separate teams, patients were booked into the INT and guided through a coordinated network of support designed to address both clinical and non-clinical needs. Weekly MDT-style triage matched patients to appropriate pathways and follow-ups have allowed us to track engagement and outcomes in real time.
Impact
Access to 60+ community services has enabled more timely support for both physical and mental health needs. We appointed two adult and one young people’s mental health practitioner, enabling INT coordinators to direct patients to appropriate support with minimal waiting times.
Our approach provides tailored, non-clinical interventions that address social, economic and psychological factors. Feedback from both patients and colleagues has consistently highlighted the quality, professionalism and empathy of the care delivered. Patients in particular value being heard, respected and supported.
We also extended the integrated model into physical health services. Advanced nurse practitioners now run cardiovascular disease (CVD) risk clinics, diabetes reviews for young patients, and in-house spirometry to clear a backlog of 9–12 months.
Outcomes
Before our initiative, we noted 379 patients attended GP appointments more than 25 times in a year, accounting for more than 14,000 consultations. After introducing our culturally sensitive model, this group made 6,000 fewer appointments over the course of a year.
A&E attendance also fell sharply. From October 2023 to March 2024, 30 frequent attenders made 1,171 visits. By the following year, from October 2024 to March 2025, the same group made just 337 visits.
There were benefits for the workforce, too. GP workload was eased through a reduction in inappropriate appointments. Clear triage and referral protocols improved team clarity, and morale has risen as staff saw the impact of personalised care. And care coordinators, ANPs, and other ARRS roles felt empowered by their new responsibilities and autonomy.
The integrated physical health services have also been successful. The in-house spirometry service cleared the backlog of 65 patients who’d been on a North East London NHS Foundation Trust waiting list for 9-12 months. It then saw other patients who needed the service, seeing a total of 257 between December 2024 and March 2025.
The high-risk patients reviewed by ANPs for CVD and diabetes saw a 50% improvement in outcomes, with many engaging successfully in preventative plans.
Future
The PCN has shown that system-wide collaboration is both achievable and effective even within existing constraints. By building trust between partners, empowering non-medical staff and using real-time data, we have delivered measurable improvements in access, outcomes and workforce sustainability.
Our integration efforts are underpinned by shared objectives, data-sharing agreements, and a collective commitment to reducing health inequalities. This joined-up approach has improved patient outcomes, strengthened relationships across the system, and created more efficient, compassionate, and personalised care.
The impact is already being scaled locally, and we are confident this model offers replicable solutions for the wider NHS.
Tips for adopting a culturally sensitive approach to healthcare
- Data-first: Let population health data guide your focus; it will reveal hidden burdens and duplication.
- Map services: Many resources already exist. Knowing them and how to refer is half the battle.
- Trust matters: Relationships across sectors need time and respect to grow.
- ARRS flexibility: Empower non-clinical staff. They are essential to capacity and sustainability.
- Start small: Piloting with three surgeries gave us fast feedback and built confidence.
- Shared language: Creating joint triage templates and referral flows simplifies MDT working.
- No extra funding: Innovation is possible with what you already have.
This is one of 10 PCNs shortlisted for PCN of the Year at the General Practice Awards. The winners will be revealed at the awards ceremony on Friday 5 December at the Novotel London West. If you’d like to be there on the night you can find out more here and book tickets here.
